Poster Presentation Annual Meetings of the Endocrine Society of Australia and Society for Reproductive Biology and Australia and New Zealand Bone and Mineral Society 2016
Periodic allergy (#363)
A 35-year old female presented to ED with anaphylaxis following ingestion of cheese, salami and avocado though she had no known intolerance to these foods. Due to symptom severity an adrenaline infusion was required. Her menstrual period began that night. Her medical history included asthma, allergic rhinitis, dermatographia and allergies to peanut, dogs and house dust mite. She had experienced two anaphylactic episodes, requiring intramuscular adrenaline, in the preceding 12 months with no obvious precipitant.
In the following six months, the patient had six further anaphylactic reactions with no clear precipitant. Prior to each event, she noticed worsening of her asthma and dermatographia. Tests for other food allergies were negative and radioallergosorbent (RAST) testing revealed a moderate response to Alternaria fungus only. Complement levels were normal and there was no family history of hereditary angioedema.
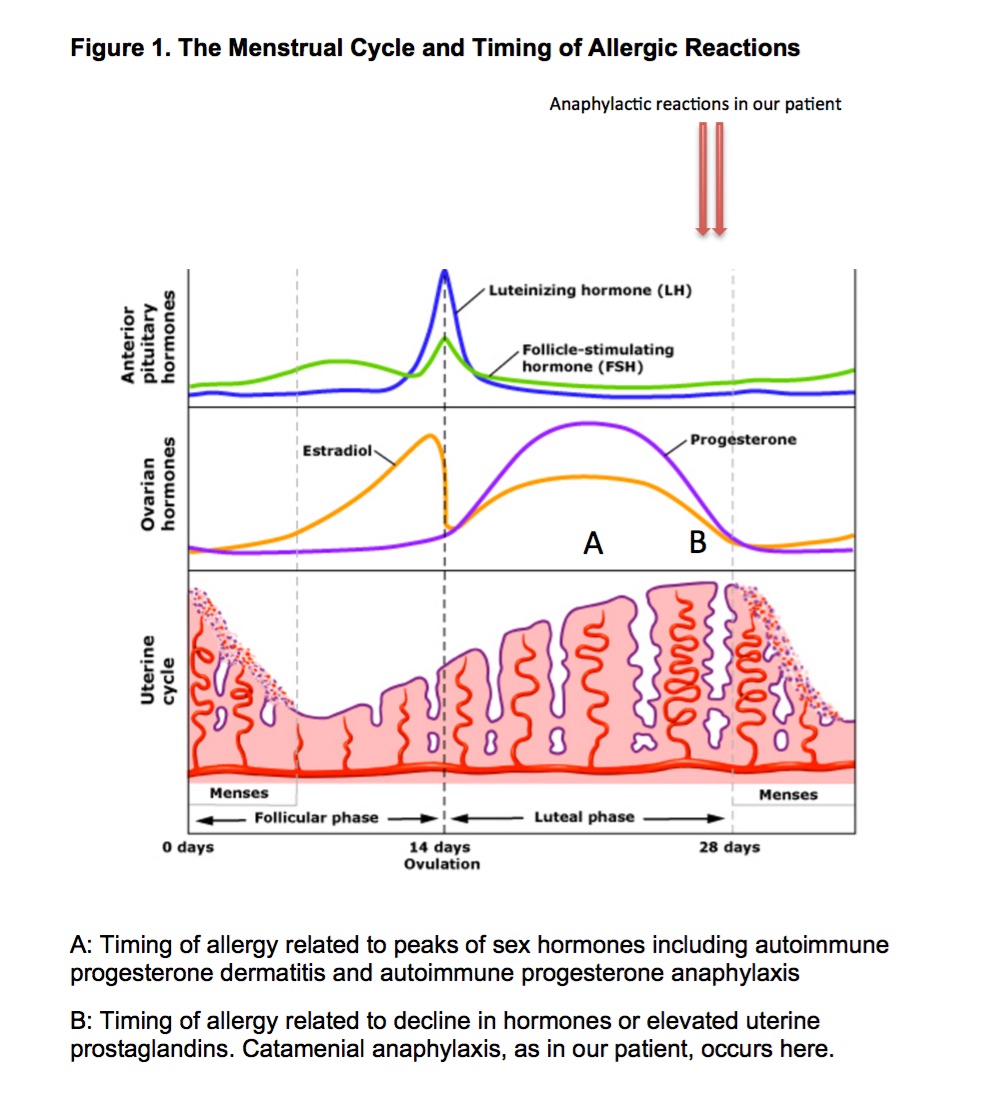
Given the lack of obvious trigger, the patient kept a diary revealing episodes all occurred just prior to the onset of menses (days 26-29). No new medications nor dietary precipitants were identified.
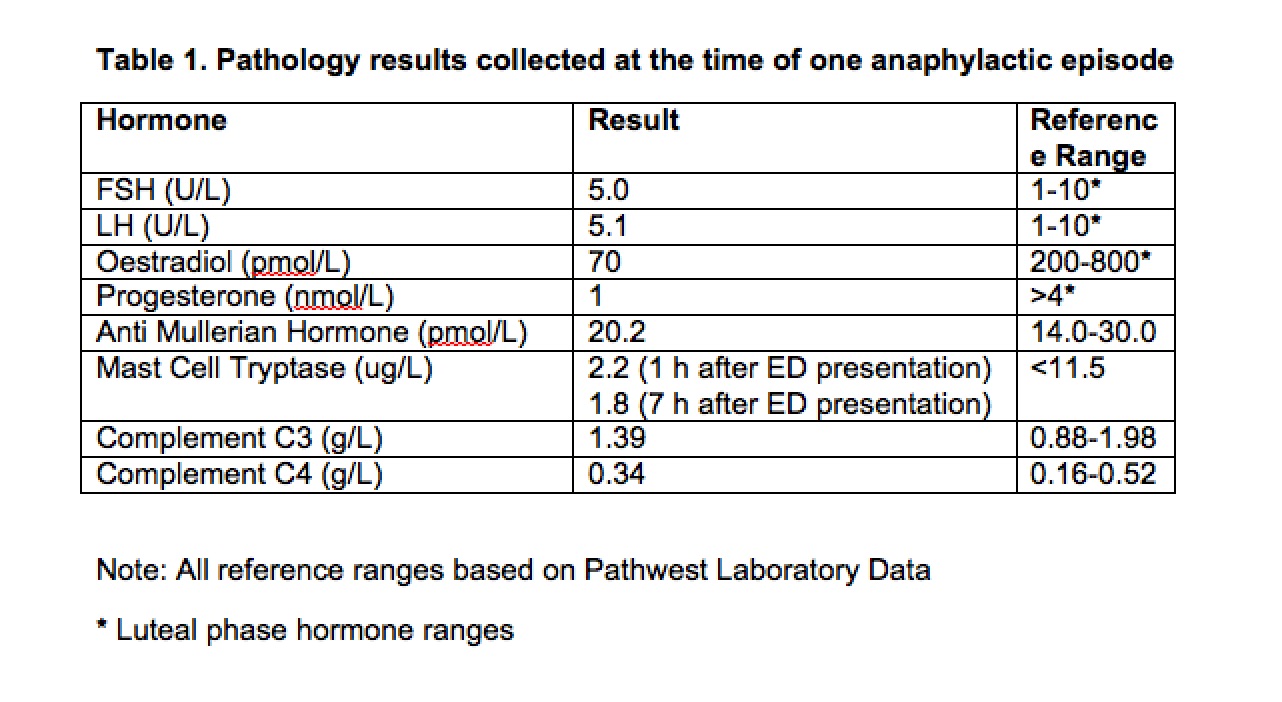
Bloods collected during one episode, revealed low oestradiol and progesterone levels. Premenstrual transdermal oestradiol was commenced from day -6 before menses continuing for 3 days into her period. She remained symptom free for 6 months. Following self-cessation of therapy she suffered two further anaphylactic reactions, again prior to menses. Oestrogen therapy was reinstituted and she remains well-controlled 15 months later. Symptom resolution with exogenous oestrogen suggests that oestrogen decline was the inciting factor in this case.
Catamenial anaphylaxis is a rare condition characterised by multisystem allergic response occurring around the time of menstruation. Diagnosis requires thorough history of the exact timing of symptoms, exclusion of other allergic triggers and response to proof of concept treatment.