Poster Presentation Annual Meetings of the Endocrine Society of Australia and Society for Reproductive Biology and Australia and New Zealand Bone and Mineral Society 2016
Bone mineral density in diabetes and impaired fasting glucose (#325)
Diabetes is associated with increased skeletal fragility and increased bone mineral density (BMD), yet the relationship between impaired fasting glucose (IFG) and BMD has not been examined. This study aimed to describe the relationship between BMD and normoglycaemia, IFG and diabetes.
Methods: This study included 863 women, 971 men, aged 20-80 years, enrolled in the Geelong Osteoporosis Study. Using multivariable regression, relationships between dysglycaemia and BMD at the femoral neck (FNBMD) and lumbar spine (LSBMD) were examined, adjusting for age, BMI and other variables. IFG was fasting plasma glucose (FPG)≥5.5mmol/L; diabetes FPG≥7.0mmol/L, use of antihyperglycaemic medication and/or self-report. As there was a BMI*dysglycaemia interaction, data were stratified by BMI cut points (women:30kg/m2, men:25kg/m2).
Results: In premenopausal women (n=417), there was no relationship between dysglycaemia and BMD. In non-obese postmenopausal women (n=297, age 64.6±9.15years), there was a non-significant 5.5% higher FNBMD in diabetes versus normoglycaemia. In IFG, FNBMD was not different from normoglycaemia whereas LSBMD was 7.1% greater. By contrast, LSBMD was 9.3% greater in diabetes versus normoglycaemia. In obese postmenopausal women (n=149, 64.8±8.74years), FNBMD was no different in IFG but was 9.0% greater in diabetes versus normoglycaemia. LSBMD was no different in IFG, but was 10.4% higher in diabetes versus normoglycaemia.
In men (55.5±16.4years), FNBMD was lower in IFG (2.7%) and diabetes (3.8%) whereas LSBMD was somewhat higher. These differences did not persist when adjusted for age and BMI (Table 1).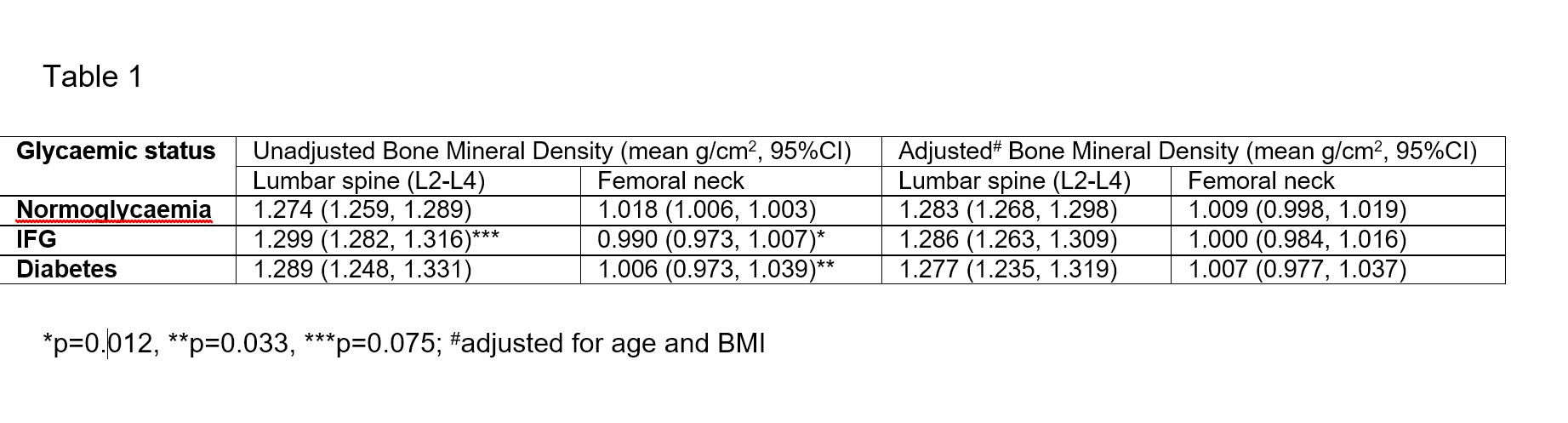
Conclusions: We confirm previous observations that BMD is higher in Type 2 diabetes, which likely constitutes the majority of our postmenopausal diabetic women. This is the first study to examine BMD in IFG and shows LSBMD, alone, is greater in postmenopausal women. Unadjusted male LSBMD was higher in IFG and diabetes compared to normoglycaemia. Analysis of the relationship between fractures and IFG and diabetes would provide clinically relevant information.